How is a histological report created?
From tissue specimen to diagnosis
Steps to the finished report

Human cells begin to break down after they are removed. To allow an optimal assessment of the tissue, it must be fixed promptly after removal, ideally without altering the structure of the cells.
For this reason, tissue specimens are not simply sent "dry" but immersed in a fixative solution. Classically, formalin (a buffered 4–10 % formaldehyde solution) is used for this.
Depending on the size of the specimen, the fixation process takes from a few hours to more than a day.

Many specimens cannot be embedded immediately. Particularly with large excisions and surgical specimens, the trained eye of a pathologist is needed to select representative portions of the overall specimen. Macroscopic assessment of the resection margins and the marking of the margins are also part of this.
Because this is an extremely important step in the entire process, it is always carried out by a pathologist with the assistance of a medical technical assistant.
Internal protocols for common tumours ensure a consistently high quality here.

During grossing, the specimens were placed in plastic cassettes. Depending on the specimen, this can produce between 1 and 100 or more cassettes. To make the tissue "sectionable", it must be post-fixed, "dehydrated" and made permeable to paraffin.
This is achieved through ascending series of alcohol and xylene. The tissue is then embedded in paraffin or acrylic resins to achieve the greatest possible consistency and stability of the tissue for the sectioning process.
These steps usually take place overnight in the tissue processor. Small specimens submitted in the morning can also be embedded, sectioned and reported in a rapid programme, so that a diagnosis can be made within the same day.
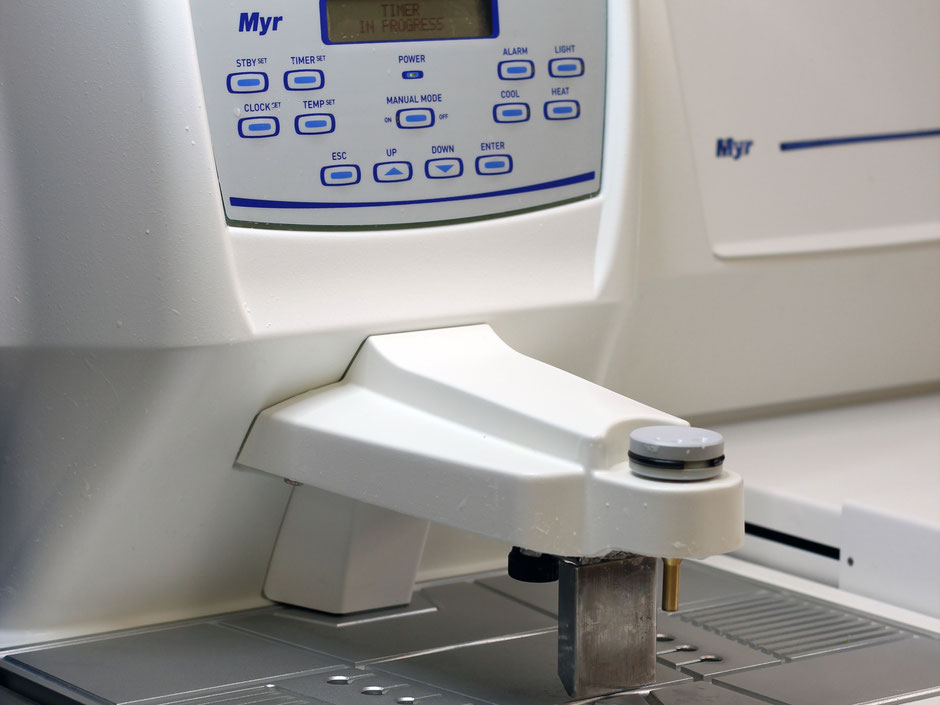
At an embedding station, the tissue pieces saturated with paraffin are placed in a metal mould, covered with hot paraffin and cooled into a wax block. The plastic cassettes serve as the block carrier.
The tissue is arranged so that the surface to be sectioned lies at the bottom. After the paraffin has cooled, the block is released from the mould. The tissue piece is now embedded in paraffin and "sticks" to the outside of the plastic cassette.

Ultra-thin paraffin sections can only be produced with precision technology. Our rotary microtomes have a holder for the block, a blade and a mechanism to control the section thickness.
The block is brought to just below the cutting plane of the firmly clamped blade. Then the desired sections of 2 to 7 µm thickness are cut and transferred into a warm water bath. The sections are then mounted onto slides, sorted into racks according to the staining required, and kept to dry in a 37 °C incubator until staining.

To make the different structures of the tissue more clearly visible, the tissue sections must be stained.
The standard stain is the so-called H&E stain (haematoxylin/eosin). Haematoxylin stains mainly nuclear structures, and eosin stains components of the cell plasma. Special stains for marking mucins, the iron detection reaction or the Giemsa stain also broaden the spectrum.
"Hand staining" is used in particular for rare special stains. All standard stains are carried out in a staining machine.
In the final step, the stained tissue sections are fitted with a very thin glass coverslip. This too is done by a machine. The specimens are thereby made more durable, and the tissue samples can be examined under the microscope without the ultra-thin sections being damaged.

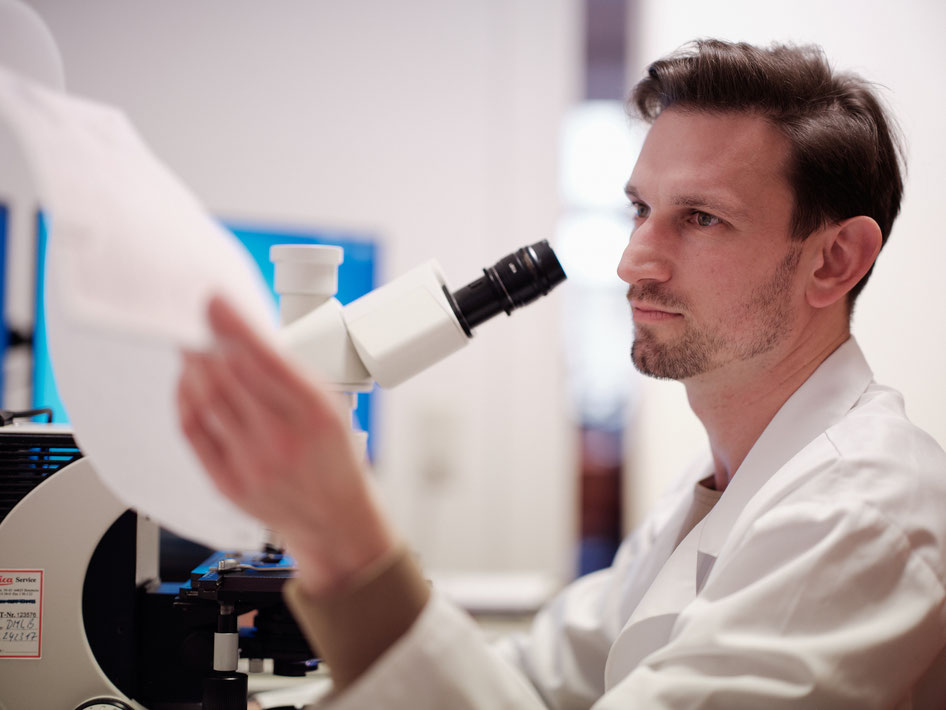
Now the finished sections can be viewed under the microscope and a diagnosis made. Various magnification levels from 16x to 1000x make it possible to identify even the smallest portions of the tissue.
Bacteria and even individual organelles of cells can be examined distortion-free with the optics of modern microscopes.
In addition, there are special optical procedures, such as polarisation filters, to make birefringent structures (foreign bodies, cholesterol crystals, calcium deposits) visible.
Live measurement and counting of distances (resection margin) and cells (e.g. coeliac diagnostics) are also used here. For this we use the latest camera and computer technology.
The reports are now written, corrected and signed in our typing office. They are available electronically at any time.
The report letters are usually sent by post. Transport via our driver service, email over secure medical networks and fax are also possible.